White Paper: Multi-Channel ePRO and Clinical Decision Support
Executive Summary
EVAL Health is a no-code electronic patient-reported outcomes (ePRO) and clinical decision support (CDS) platform that addresses critical regulatory, financial, and operational challenges: meeting CMS quality reporting and post-acute monitoring requirements, capturing value-based care incentives, reducing manual documentation burdens, and deploying assessment tools without lengthy IT development cycles. Launched mid-2025, the platform enables healthcare organizations to deploy validated assessment instruments across multiple channels with unified data capture and seamless EHR integration.
Key Capabilities:
- Multi-Channel Delivery: Deploy the same assessment across SMS, email, kiosk, and clinician-administered channels, targeting 65-74% completion rates.
- Automated Longitudinal Monitoring: Scheduled patient assessments with clinical priority escalation for proactive chronic disease management and regulatory compliance.
- Rapid No-Code Configuration: Deployment in days-to-weeks, representing an 85-93% reduction in time compared to traditional EHR development
The Healthcare IT Challenge
Healthcare organizations face interconnected obstacles in implementing patient assessment and clinical decision support systems:
1. Channel Fragmentation
Single-channel approaches limit accessibility and reduce completion rates. Email-only surveys achieve 43-50% completion; SMS-only achieves 50-67%. Organizations using separate systems face data fragmentation and inconsistent scoring.
2. Manual Workflow Burdens
Traditional workflows require significant manual effort: paper form transcription, manual scheduling, phone calls for non-responders, and tracking which patients are due for assessment. Each manual step introduces error risk and consumes clinical staff time.
3. Extended Development Cycles
Traditional EHR-based assessment tool development requires 6-12 months involving scarce IT resources. This delays implementation of new clinical guidelines and discourages optimization.
Regulatory and Financial Drivers
Healthcare organizations face increasing regulatory requirements and financial incentives tied to patient-reported outcomes and longitudinal monitoring.
1. CMS Quality Payment Programs
MIPS and Alternative Payment Models tie significant Medicare reimbursement to quality performance, with organizations facing payment adjustments of ±9% (scaling to ±12% by 2027). Many measures specifically require systematic PRO collection.
2. Post-Acute Care Monitoring Requirements
CMS mandates systematic post-discharge monitoring. HRRP imposes penalties up to 3% of Medicare payments for excess readmissions. HAC Reduction Program can reduce payments by 1%. Systematic PRO monitoring provides early warning and supports timely intervention.
3. Value-Based Care Contracts
ACOs, bundled payments, and commercial value-based contracts require systematic outcome tracking. Organizations lacking structured PRO infrastructure struggle to demonstrate performance and risk contract penalties.
4. Staffing Efficiency Imperatives
Personnel costs comprise 50-60% of healthcare operating expenses. Manual monitoring workflows consume significant clinical time. Automation directly impacts operational sustainability.
EVAL Health Solution
1. Multi-Channel ePRO Delivery with Unified Architecture
EVAL deploys identical assessment instruments across all channels simultaneously:
-
Remote Digital (SMS/Email): Automated delivery before appointments
-
Waiting Room Kiosk: Dedicated tablets for early-arriving patients
-
Clinician-Administered: Provider tablets for assisted completion
All channels access the same assessment definition, ensuring identical question presentation, response capture, and scoring. Results can be written to the EHR from any channel upon review and approval.
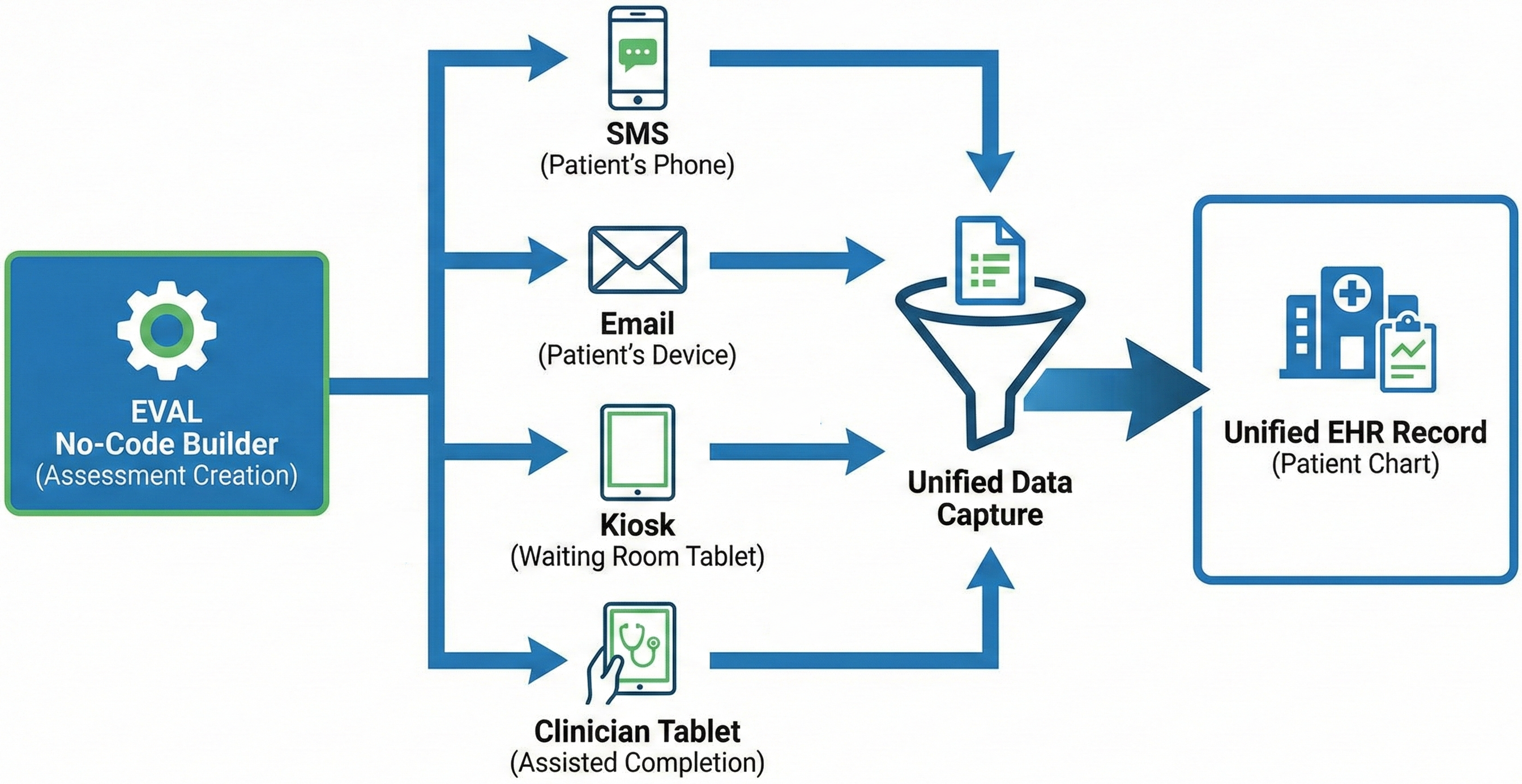
Figure 1: EVAL Multi-Channel Architecture. A single assessment built in the no-code builder is delivered across multiple channels, with all data funneling back into a unified EHR record.
Research on multi-channel delivery demonstrates significant completion rate improvements. A perioperative outcomes study (Romeiser et al., 2021) comparing email-only, SMS-only, and concurrent mixed-mode approaches found preoperative completion rates of 74.4% for concurrent delivery versus 43.1% for email-only and 67.1% for SMS-only. At 7 days postoperative, concurrent delivery achieved 66.9% versus 46.8% (email) and 50.0% (SMS). At 30 days, rates were 65.0% versus 43.1% and 49.5% respectively. Concurrent multi-channel delivery yielded 3.4x higher odds of response versus email alone and 1.9x higher odds versus SMS alone, with particular effectiveness for traditionally difficult-to-reach populations including non-White patients, older individuals, and those not in partnerships.
Clinical applications include routine screening programs (depression, fall risk, substance use), perioperative care (pre-surgical assessment, post-discharge recovery), and chronic disease management (monthly symptom monitoring).
2. Automated Longitudinal Monitoring with Clinical Escalation
EVAL provides an automated workflow designed to significantly reduce or eliminate manual burden. The platform's scheduled delivery engine triggers assessments automatically based on fixed intervals. Clinical priority escalation provides automated analysis with configurable alert thresholds, generating immediate alerts in the EHR (where supported) and email notifications to designated providers.
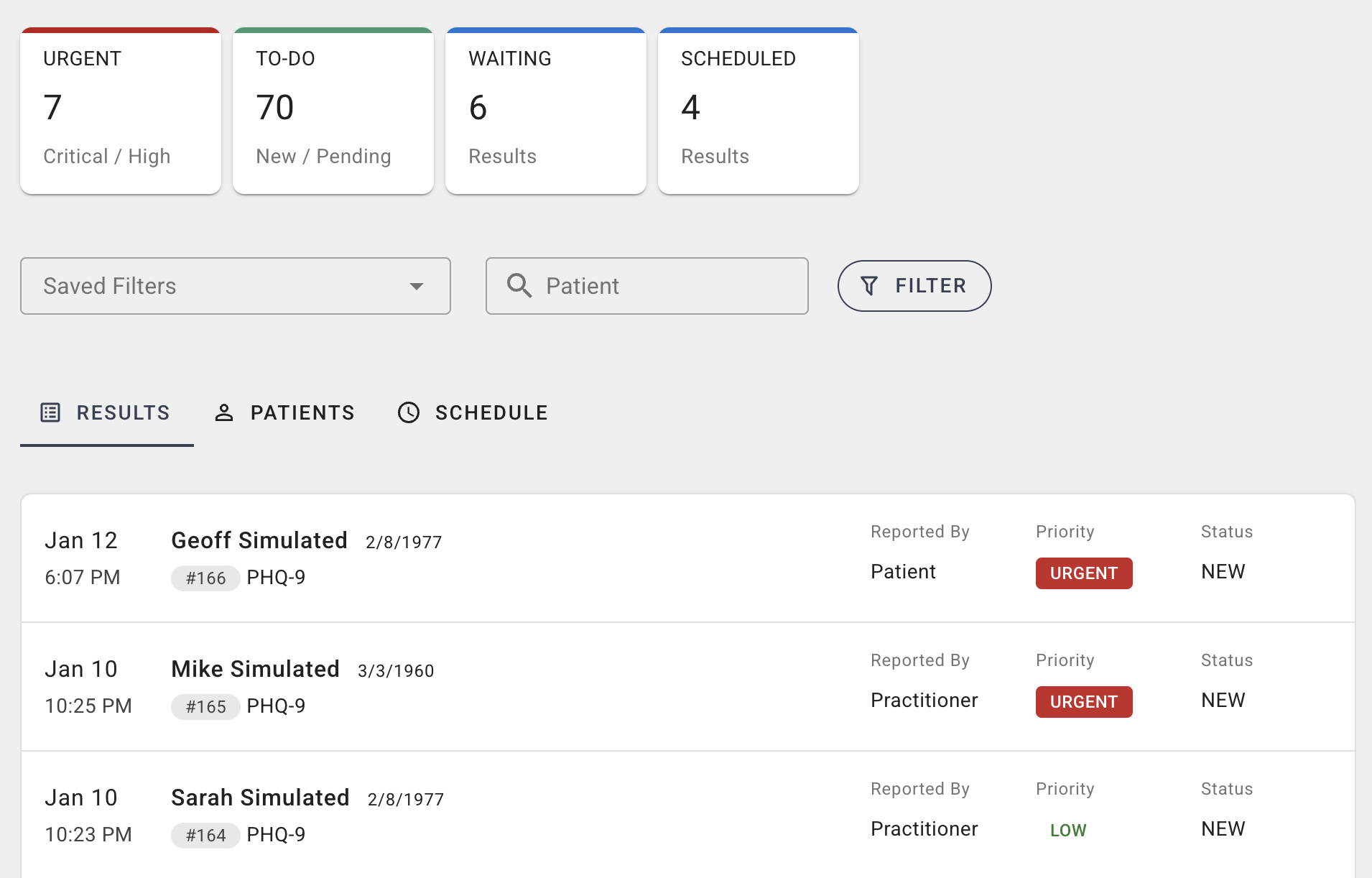
Figure 2: EVAL Clinical Dashboard. Custom panels aggregate patient activity and results with advanced filtering. High-priority items are flagged with URGENT status, allowing clinicians to identify deteriorating patients at a glance and initiate proactive outreach.
This approach is expected to enable 2–4 week earlier detection of treatment non-response or clinical deterioration compared to appointment-only assessment. Early intervention supports multiple organizational priorities:
-
Quality Metric Achievement: Demonstrates care effectiveness for MIPS and value-based contract reporting
-
Regulatory Compliance: Meets CMS requirements with automated documentation
-
Appropriate Care Delivery: Addresses complications before escalation
-
Risk Stratification: Identifies high-risk patients requiring intensified coordination
Evidence from similar automated monitoring programs in chronic disease management suggests potential 20-30% reduction in preventable acute care utilization when systematic PRO monitoring is combined with established clinical response protocols.
3. Rapid No-Code Configuration
Traditional EHR custom development requires 6-12 months with full development teams, requiring scarce IT resources and creating vendor lock-in. EVAL provides a visual no-code configuration interface enabling authorized users to build and deploy assessment tools without traditional software development. The platform includes a web-based visual form builder, point-and-click logic configuration, and clinical decision rules for alert thresholds.
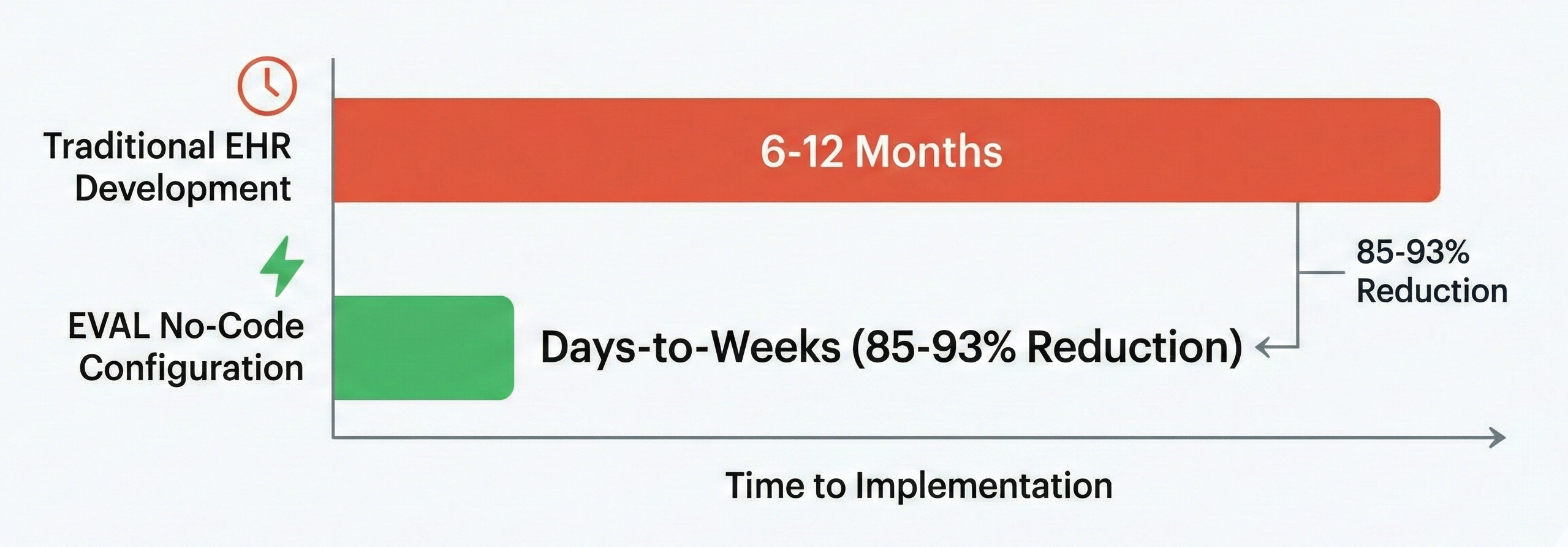
Figure 3: Implementation Time Comparison. EVAL's no-code platform significantly reduces the time to deploy clinical assessments compared to traditional EHR development cycles.
Industry research (Uliyar & Harper, 2025) establishes that traditional EHR custom workflows require 6-12 months, while low-code/no-code platforms reduce this to 4-8 weeks—an 83-93% time reduction. Research on EHR-agnostic platforms (Solomon et al., 2023) demonstrates that vendor-neutral approaches can achieve high adoption (77.8%) while simplifying development.
The EHR-agnostic architecture enables CDS tools to be deployable across multiple EHR environments (Epic, Cerner, Meditech), supports multi-site research studies without redundant development, uses standards-based integration (HL7 FHIR) rather than vendor-specific APIs, and allows institutional mergers without tool redevelopment.
Clinical and Financial Applications
The rapid configuration capability enables diverse high-value use cases that directly impact organizational financial performance:
-
Quality Reporting Programs: Deploy and modify MIPS-required measures without IT backlog; adapt to annual specification changes in days versus months
-
Clinical Research Infrastructure: Support grant-funded studies and pharmaceutical partnerships; rapid deployment maintains research timelines and protects institutional revenue
-
Specialized Clinical Programs: Rare disease registries, precision medicine, and Center of Excellence programs differentiate capabilities and attract complex case referrals
-
Value-Based Contract Support: Deploy condition-specific monitoring protocols required by ACO, bundled payment, and commercial value contracts without IT dependency
This flexibility addresses a critical strategic gap: traditional EHR customization cannot keep pace with evolving quality programs, new contract requirements, or emerging clinical evidence. Organizations can adapt assessment protocols in days-to-weeks rather than waiting 6-12 months for scarce IT resources or vendor development cycles.
Why Integrated Multi-Channel ePRO + No-Code CDS + EHR Matters
Traditional approaches force organizations to choose one of:
- Best-in-class ePRO platforms (but lacking CDS)
- EHR-native tools (with CDS but poor patient experience)
- Custom development (integrated but expensive and slow)
EVAL uniquely combines all three capabilities in a single platform, eliminating the integration burden and data fragmentation of multi-vendor approaches
Expected Outcomes
Based on EVAL's technical capabilities and industry evidence, organizations can anticipate improvements across operational efficiency, clinical quality, and patient experience.
Operational efficiency: Targeting 30-50% reduction in staff time for assessment tasks through elimination of paper transcription, automated delivery versus manual phone calls, and real-time EHR documentation. Multi-channel delivery targeting 65-74% completion rates versus 43-67% for single-channel approaches. Deployment in days-to-weeks versus 6-12 months represents an 85-93% reduction in time-to-implementation.
Clinical quality: Automated longitudinal monitoring enables 2-4 week earlier detection of treatment non-response or clinical deterioration. Proactive management potentially achieving 20-30% reduction in preventable acute care utilization when combined with established clinical protocols.
Patient experience: Convenience and flexibility expected to yield 15-20% improvement in patient satisfaction scores. Regular automated check-ins demonstrate clinical team engagement.
Use Case Example 1: Perioperative Multi-Channel ePRO for Surgical Recovery
Clinical Context
A surgical program wants to track post-operative recovery quality and identify patients experiencing complications. The current approach relies on phone calls at set intervals, achieving poor completion rates (40-50%), missing patients between scheduled calls, and consuming significant nursing time.
Regulatory and Financial Context
CMS requires systematic post-discharge outcome monitoring through multiple programs. HRRP imposes Medicare payment penalties up to 3% for excess readmissions. MIPS surgical specialty measures incorporate patient-reported functional outcomes. Value-based surgical bundles require documented patient-centered outcome assessment.
Traditional phone-call follow-up creates compliance gaps: inconsistent completion rates, retrospective data, manual documentation burden, and inability to demonstrate systematic monitoring protocols.
The Challenge: Traditional Single-Channel Approach
Nurses manually call patients at 7 and 30 days post-surgery. Many patients don't answer, requiring multiple callbacks. Patients recall recovery inconsistently. No systematic screening between scheduled intervals. Nurses spend 15-20 minutes per patient on calls and documentation.
This approach often has low completion rates (40-50% at 7-day, 30-40% at 30-day), missed opportunities for early complication detection, labor-intensive process, inconsistent documentation quality.
EVAL Implementation: Multi-Channel ePRO Approach
-
Preoperative Assessment: 3 days before surgery, automated QoR-15 baseline sent via patient's preferred channel (SMS, email, or tablet at pre-op appointment).
-
Post-Operative Monitoring: Days 1, 3, 7, 14, 30 - automated QoR-15 delivered via same channel with optimal timing, automated reminders, and escalation to phone call only if digital non-response after 48 hours.
-
Real-Time Clinical Escalation: Immediate alerts for concerning responses (severe pain, infection signs, shortness of breath, distress). Alert routing based on urgency to nurse navigator, same-day call, or immediate surgeon paging.
Expected Benefits
Completion Rates (Romeiser et al., 2021)
- Preoperative: 74% (vs. 43% phone-only)
- 7-Day: 67% (vs. 47% phone-only)
- 30-Day: 65% (vs. 43% phone-only)
Operational Efficiency
- Nursing time reduced from 15-20 min/patient to 2-3 min for flagged patients only (75-85% reduction)
- Automated documentation eliminates manual transcription
Clinical Quality and Regulatory Compliance
- Earlier complication detection through continuous monitoring (target: 1-2 weeks earlier than appointment-only)
- Systematic PRO collection supports MIPS measures and bundle reporting
- Earlier intervention supports HRRP readmission prevention
- Regular check-ins improve patient experience (25% of MIPS Quality category)
Financial Impact Traditional phone-based monitoring for 200 patients/month requires ~1.0-1.35 FTE nursing time. Automated alert-based review reduces this to 0.15-0.25 FTE—representing approximately $60K-90K annual savings or cost avoidance for program expansion. Enables scaling to meet quality requirements without competing for scarce nursing resources.
What This Means for Clinical Practice
| Traditional Phone Calls | EVAL Multi-Channel ePRO |
|---|---|
| Fixed timing (7-day, 30-day) | Flexible assessment schedule (daily if needed) |
| Nurse initiates contact | Patient completes when convenient |
| 40-50% completion rate | 65-75% completion rate |
| 15-20 min per patient | 2-3 min per flagged patient |
| Retrospective recall | Real-time reporting |
| Business hours only | 24/7 availability |
| Single attempt or multiple callbacks | Automated reminders |
| Manual documentation | Auto-documented in EHR |
The surgical program can now:
-
Scale monitoring from 50-75 to 200+ patients/month with same resources
-
Respond proactively to concerning patterns before they become emergencies
-
Focus nursing time on patients with alerts versus routine check-ins for all
-
Improve quality metrics with higher completion rates for MIPS and payer contracts
-
Meet CMS mandates with systematic post-op monitoring infrastructure
Use Case Example 2: Integrated Behavioral Health in Primary Care
Clinical Context
A primary care practice implements universal depression screening per USPSTF guidelines, requiring annual screening and longitudinal monitoring for patients on treatment. Current paper-based approach results in poor completion rates (45%), data fragmentation, and missed longitudinal trends.
The Challenge: Paper-Based Fragmented Monitoring
Manual transcription of paper scores, delayed response (clinicians only see results during visits), and no systematic way to track PHQ-9 score changes over treatment.
EVAL Implementation: Automated Behavioral Health Workflow
-
Initial Screening: PHQ-9 automatically sent via email/SMS 24 hours before annual physical. Patients without digital access receive clinician-administered PHQ-9 on tablet during rooming.
-
Treatment Monitoring: Patients starting antidepressants receive automated PHQ-9 every 2 weeks via email/SMS.
-
Smart Alert Routing: Immediate alert to Care Manager if suicidal ideation item is positive or score indicates severe distress.
Expected Benefits
-
Higher Screening Rates: 85%+ completion vs. 45% paper-only
-
Earlier Detection: Treatment non-response identified 2-4 weeks earlier than standard 2-3 month follow-up
-
Operational Efficiency: Reduced care manager time on manual outreach
-
Improved Quality Metrics: Better payer contract performance through systematic documentation
-
Enhanced Referral Management: Systematic screening with automated scoring optimizes internal referrals to psychiatry/therapy for integrated systems, strengthens value-based contract performance for independent practices, and meets CCBHC collaboration requirements
Limitations and Considerations
Scope of Time Savings: Rapid configuration addresses technical setup. Total timeline including clinical validation, workflow design, pilot testing, and training: 6-8 weeks typical.
Complexity Variance: Simple instruments (PHQ-9) show 95%+ time reduction. Moderate complexity (branching logic) shows days-to-weeks deployment. High complexity workflows are still faster than traditional (70-85% reduction).
Organizational Readiness: Success requires clear clinical requirements, adequate informaticist resources, governance for tool approval, and technical infrastructure for EHR integration.
Pre-Clinical Practice Deployment Status: As of January 2026, EVAL Health is entering production clinical practice deployment with initial sites anticipated live within 1-3 months. Expected benefits are based on published evidence, internal pilot testing, analogous systems in peer-reviewed literature, and industry benchmarks. Real-world clinical outcomes data will be collected and reported as production implementations generate evidence.
Conclusion
Healthcare organizations require patient assessment and clinical decision support tools that meet regulatory requirements, capture financial incentives, accommodate diverse patient populations, integrate seamlessly into clinical workflows, and can be rapidly deployed as clinical guidelines evolve. Traditional approaches create barriers through single-channel implementations, manual coordination burdens, and 6-12 month development cycles—limiting organizations' ability to respond to CMS quality program requirements and value-based care contracts.
EVAL Health addresses these interconnected challenges through an integrated platform that combines multi-channel ePRO delivery (targeting 65-74% completion rates based on published research), automated longitudinal monitoring with clinical escalation (enabling proactive chronic disease management and regulatory compliance), and rapid no-code configuration (reducing deployment timelines by 85-93%). These capabilities deliver operational efficiency through staffing optimization, improved clinical quality through earlier detection of patient trends, enhanced regulatory compliance through systematic documentation, and improved patient experience through convenient multi-channel access.
As an emerging platform entering production clinical deployment in early 2026, EVAL Health represents alignment with evidence-based best practices in ePRO implementation while addressing known barriers to adoption and sustainability. The platform's focus on regulatory compliance, financial incentives, and operational efficiency positions healthcare organizations to meet evolving quality requirements while optimizing resource utilization.
About EVAL Health
EVAL Health is a healthcare technology company focused on making patient-reported outcomes and clinical decision support accessible to healthcare organizations of all sizes. Our platform combines multi-channel patient engagement, automated workflow management, and rapid no-code configuration to address the practical barriers that have historically limited ePRO adoption.
The platform launched in mid-2025 and is currently being deployed with initial clinical partners for production use with live patients.
Updated about 2 months ago